For Medicaid-Insured Patients with Cancer, Health Insurance Does Not Always Mean Health Access < Yale School of Medicine
Although there has been a significant increase in the number of U.S. residents insured through Medicaid since the expansion of the Patient Protection and Afforadble Care Act (ACA) in March 2010, the ability of Medicaid-insured patients to access cancer care services has not been well understood. In a study published today in the journal JAMA Network Open, researchers at Yale Cancer Center assessed the acceptance of Medicaid insurance among patients diagnosed with common cancers.
“We found that Medicaid acceptance differed widely across cancer care facilities, with a substantial number of centers not offering services to patients with Medicaid insurance,” said Michael Leapman, MD, MHS, Associate Professor of Urology, Clinical Program Leader for the Prostate & Urologic Cancers Program at Yale Cancer Center and Smilow Cancer Hospital, and senior author on the study.
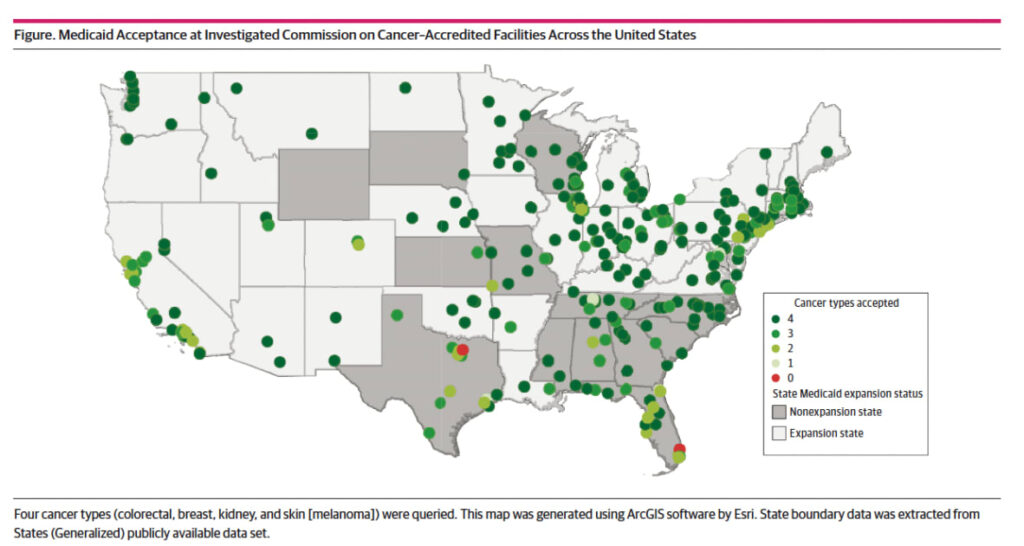
In the study led by first-author Victoria Marks, a second-year medical student at Yale, 334 Commission on Cancer-accredited facilities were sampled, of which, only 226 (67.7%) accepted new patients with Medicaid insurance for the four common cancers selected (colorectal, breast, kidney, and skin). Acceptance varied among the facilities, with 296 (88.6%) accepting Medicaid for at least three types, 324 (97.0%) for at least two, and 331 (99.1%) for at least one type. Collectively, these findings underscore the persistent gaps that exist for patients with Medicaid in utilizing services at hospitals distinguished for high-quality cancer care.
“This study underscores that having health insurance alone does not necessarily mean that patients can practically access healthcare. While major recent expansions of Medicaid have led to increases in health insurance coverage for Americans with cancer, we have to be aware and do more to ensure that insurance will actually translate to timely and high-quality care,” said Dr. Leapman.
Facilitates that were more likely than others to accept patients with Medicaid included National Cancer Institute (NCI)-designated cancer centers, 89.7% of which offered high access to patients with Medicaid, and academic centers (86.4%). Moreover, facilities located in states that expanded Medicaid were also more likely to offer high access to Medicaid patients, 71.3% versus 59.6%.
“The results of this study do not necessarily mean that patients will not be able to access care anywhere, but may require a circuitous and impractical path, and may not be seen at centers designated for cancer care,” Dr. Leapman explained.
According to Dr. Leapman, finding solutions that increase access for Americans with Medicaid will be complex. “Despite a large increase in the number of Medicaid-insured patients, most factors that limit a hospital or physician’s participation in Medicaid have not changed,” he said. “These include low reimbursement, high administrative burden, and limited specialist participation in managed care organization networks. Even modest increases in reimbursement may have a positive impact, and progress in payment structures that prioritize healthcare quality are promising as well. Still, identifying these gaps in access is an important first step that can direct awareness.”
Additional Yale authors include Michelle Salazar, Elizabeth Berger, and Daniel Boffa.
This content was originally published here.

Responses